Poorest areas of England ‘will suffer under new NHS spending formula’
Plan will see funding rise by 14 per cent for some and drop by a quarter for others
Your support helps us to tell the story
From reproductive rights to climate change to Big Tech, The Independent is on the ground when the story is developing. Whether it's investigating the financials of Elon Musk's pro-Trump PAC or producing our latest documentary, 'The A Word', which shines a light on the American women fighting for reproductive rights, we know how important it is to parse out the facts from the messaging.
At such a critical moment in US history, we need reporters on the ground. Your donation allows us to keep sending journalists to speak to both sides of the story.
The Independent is trusted by Americans across the entire political spectrum. And unlike many other quality news outlets, we choose not to lock Americans out of our reporting and analysis with paywalls. We believe quality journalism should be available to everyone, paid for by those who can afford it.
Your support makes all the difference.The poorest parts of England will have their health funding cut while affluent areas will benefit under a proposed new NHS spending formula, experts have warned.
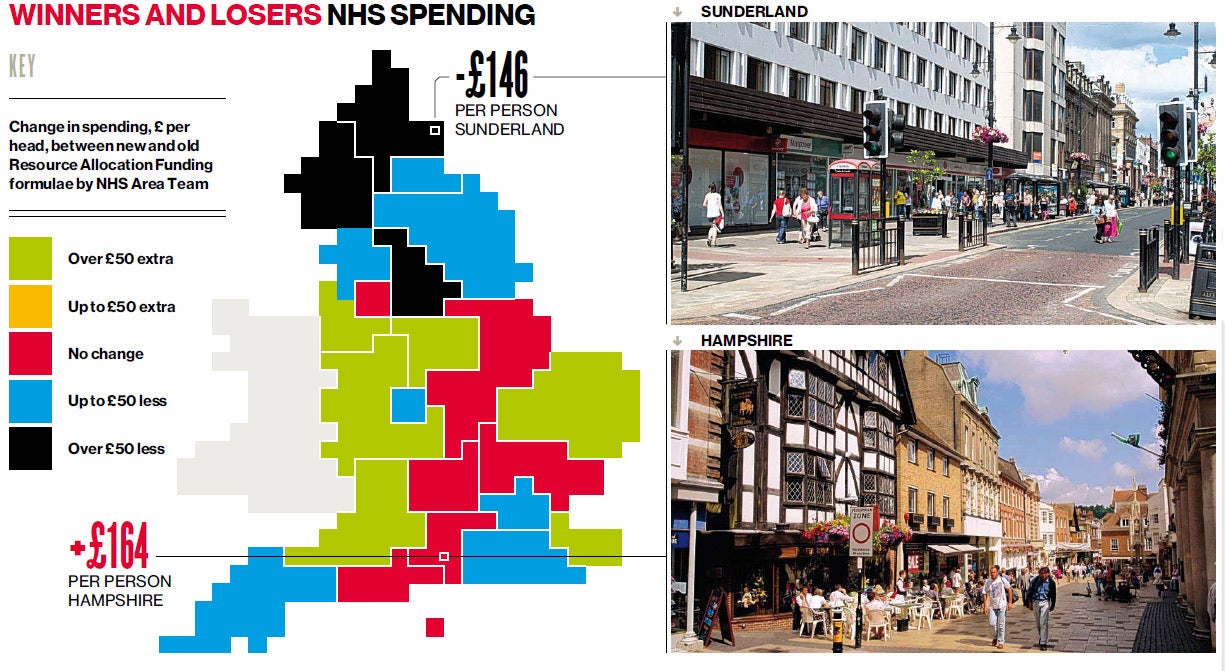
Click image above to enlarge graphic
New plans for allocating resources across England’s clinical commissioning groups (CCGs), under consideration by NHS England, would see a measure that takes deprivation into account dropped in favour of a greater emphasis on the age of the population.
But in a letter to the British Medical Journal, academics from Durham University said that, with life expectancies already higher in wealthy areas, the new formula measure could “undermine the principle of equal opportunity of access for equal need” and entrench the North-South health divide.
Using the proposed new formula to map spending across England, they found the more affluent and healthy South-east would benefit the most, while poorer, less healthy areas in the North would lose out substantially.
In one CCG, South Eastern Hamp-shire, where the healthy life expectancy for women is 68, NHS funding would increase by £164 per person under the new formula – a 14 per cent increase. By contrast, in Sunderland, where a woman’s healthy life expectancy is 58, NHS funding per person would decrease by £146 – a decline of 11 per cent.
Poorer parts of London would also lose out, they warned, with Camden receiving £273 less per head – a cut of more than a quarter on current spending.
“Although these changes are not on the scale that a purely ‘age only’ allocation formula would produce, they are still sufficient to undermine the principle of ‘equal opportunity of access for equal need,’” write Professor Clare Bambra and Dr Alison Copeland, from Durham’s Wolfson Research Institute for Health and Wellbeing.
Figures released by Public Health England earlier this year highlighted what the Health Secretary, Jeremy Hunt, called “shocking” variations across England in the number of people dying prematurely, with poorer areas, predominately in the North, performing much worse than affluent and mostly southern areas.
Hampshire was the 10th best-performing region in England for numbers of premature deaths from the four main killers: cancer, heart disease and stroke, lung disease and liver disease, with 215 premature deaths per 100,000 members of the population. Sunderland, meanwhile, came in the bottom 20 worst-performing regions with 337 early deaths per 100,000 people.
While older people usually need far more health services, concentrating health spending in areas where there are more elderly people can exacerbate existing inequalities – because it is these areas where, by definition, life expectancy will already be higher.
NHS England is currently reviewing the way it allocates funding following advice from the independent Advisory Council of Resource Allocation. The NHS allocates funding of more than £63bn to England’s 211 CCGs.
A spokesman for NHS England, said: “The funding allocations review group has been exploring and considering the best approach to ensuring that any future funding allocation proposals ensure equal access to health services across the country and address health inequalities. It is only right that as part of this process we continue to examine the risks and benefits of a range of potential options.
“CCGs’ commissioning responsibilities are only one part of the full range of NHS services commissioned, so it is vital to understand their allocations in the context of primary care, specialised services and social care, and ensure that money is targeted to the areas in which it will have the biggest impact in improving patient outcomes.”

Explainer: Funding formula
The NHS’s stated intention in allocating health funding in different parts of the country is to “provide equal opportunity of access for equal need”. The first element of the funding formula is the size of local populations, with more money being allocated the more people there are. Spending per head is then adjusted or weighted depending on different needs.
The more elderly the population, the more the need, because older people are more likely to require more hospital appointments, drugs, health visitors and other interventions. The costs of delivering healthcare in any given area are also taken into account. So in London, land and building costs will be higher than they are in Leeds, and staff costs may also be higher.
Currently, the spending formula also includes a deprivation measure: the “health inequality weighting”. It is this final measure that may be removed from the new formula – placing a greater emphasis on age-related allocation, which, experts say, risks exacerbating existing inequalities by focusing resources in areas where life expectancies are already high.
Charlie Cooper
Join our commenting forum
Join thought-provoking conversations, follow other Independent readers and see their replies
Comments